Irismar Reis de Oliveira, MD, PhD - Professor of Psychiatry, Department of Neurosciences and Mental Health, Federal University of Bahia, Brazil
TBCT is a new branch of Beckian cognitive-behavior therapy (CBT) that organizes known standard CBT and behavioral techniques into a step-by-step fashion. In developing TBCT, my goal was to make CBT easily mastered by the therapist and more easily understood by the patients. TBCT should also be simpler to be implemented and maintain CBT’s recognized effectiveness and transdiagnostic feature (de Oliveira, 2015; 2016). A detailed case illustration may be found on the Common Language for Psychotherapy Procedures website (de Oliveira, 2012a).
Inspiration for the development of TBCT came initially from the novel The Trial, by Franz Kafka (1925/1998). Although it was not the first time the courtroom metaphor was used in CBT – Freeman and DeWolf (1992), Cromarty and Marks (1995), and Leahy (2003) had already used this metaphor –, my idea was conceptualizing core beliefs (CBs) as self-accusations and giving all the columns of the traditional dysfunctional thought record (DTR) the courtroom connotation (de Oliveira, 2011). For instance, the column corresponding to the evidence confirming the CB would bring the prosecutor’s plea, and the evidence not supporting it would carry the defense attorney’s statements. The newly derived 7-column DTR, named trial-based thought record (TBTR; de Oliveira, 2008), contained several well-known traditional CBT techniques like the downward arrow approach (Burns, 1980), the sentence reversal procedure (Freeman and DeWolf, 1992), and the upward arrow technique (Leahy, 2003). A more detailed case illustration may also be downloaded on the Common Language for Psychotherapy Procedures website (de Oliveira, 2012b).
Several studies conducted in the last decade support the TBTR use in different psychiatric disorders (de Oliveira, 2008; de Oliveira, Duran, and Velasquez, 2012; de Oliveira, Hemmany, Powell, Bonfim, Duran, Novais, et al., 2012). For instance, TBTR was shown to decrease the credibility given by patients to dysfunctional negative CBs and the intensity of corresponding emotions in social anxiety disorder (de Oliveira, Powell, Caldas, Seixas, Almeida, Bomfim, et al. 2012; Powell, de Oliveira, Seixas, Almeida, Grangeon, Caldas et al. 2013). The conclusion reached by the above-mentioned studies was that TBTR might help patients reduce the credibility attached to the negative CBs and the intensity of corresponding emotions, regardless of the diagnosis.
New techniques were progressively added to the TBTR, resulting in TBCT. Such techniques were modifications of standard CBT and other approaches. Consequently, TBCT is an example of assimilative psychotherapy integration (Messer, 1992), in which various techniques from different theoretical origins are incorporated within the context of understanding provided by the home theoretical approach (Stricker, 2010). From the time of its original development, TBCT relied on Beckian CBT as the organizing theory, and subsequently added technical interventions drawn from several other approaches. Among them were Gestalt, compassion-focused therapy, metacognitive therapy, mindfulness, and Mitchell’s (1988) two-person relational model.
TBCT has its own case conceptualization, which makes it an individualized approach. It is divided into 3 levels and 3 phases, and includes a cyclic interactional mechanism in which components in each level influence the others, and flexibly allow the therapist to adapt the treatment to the individual’s features (de Oliveira, 2016).
Figure 1 depicts the three levels of information processing in the TBCT conceptualization diagram, and shows how a situation that is appraised in a biased fashion by the automatic thought (AT) elicits a dysfunctional negative emotion, which, in turn, produces undesired consequences in terms of behaviors and/or physiological responses. Figure 1 also contains arrows pointing back to the emotion, ATs and the situation, meaning that a confirmatory bias might preclude re-examination of the situation and replacement of the incorrect ATs with more functional and healthier perceptions (de Oliveira 2015; 2016).
Figure 1. TBCT case conceptualization diagram, phase 1, and its 3-level cognitive components: ATs, UAs and CBs. Here, dysfunctional negative CBs are predominantly active.
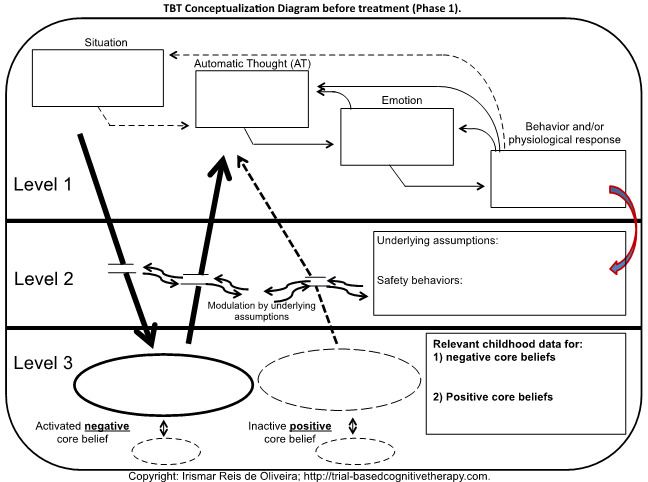
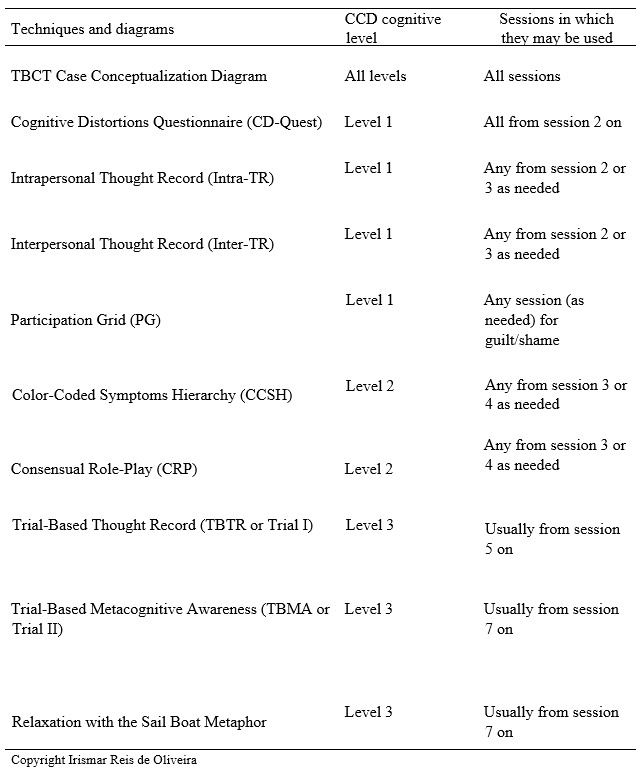
The TBCT case conceptualization diagram was also designed to help the patient realize that the behaviors that decrease anxiety and produce relief (e.g., avoidance) are little by little converted into coping strategies or safety-seeking behaviors, shown in Figure 1 as an arrow directed from the behavior and physiological response from the first to the second level on the right-hand side of the picture, meaning that situational perceptions in the first level (ATs) are progressively transformed into underlying assumptions (UAs) at the second level, which maintains and is maintained by the coping strategies/safety behaviors (de Oliveira, 2016). The table below shows the tools that were developed and are currently used during the TBCT therapy course.
Table 1. TBCT techniques and its diagrams. Column 2 informs the cognitive levels and column 3 informs in which sessions they are usually used (de Oliveira 2016).
The main TBCT technique used to restructure cognitions in the third level, namely CBs (Figure 1), is the TBTR. Besides including a courtroom metaphor, it introduces at least 12 known techniques usually used in CBT and listed below (de Oliveira, 2016):
- Socratic dialogue;
- Guided discovery;
- Imagery re-scripting;
- Empty chair or chairwork;
- Downward arrow technique (investigation);
- Evidence supporting the negative CB (prosecutor’s first plea);
- Evidence not supporting the negative CB (defense attorney’s first plea);
- Eliciting more automatic thoughts by discounting the positives (prosecutor’s second plea);
- Sentence reversal (defense attorney’s second plea);
- Upward arrow technique to uncover positive CBs (the defense attorney goes deeper);
- Identifying cognitive distortions (jurors’ phase); and
- The positive data log (preparation for the appeal), during which the patient summons the inner defense attorney as an ally to distance oneself even more and to collect daily elements that support the newly activated functional positive CBs.
In summary, TBCT is an evidence-based, three-level and three-phase Beckian branch of CBT, whose main techniques use the courtroom metaphor, and designed to facilitate the work of the therapist and the client by means of a highly structured (although flexible) protocol.
Burns, D.D. (1980). Feeling Good: The New Mood Therapy. New York: Signet.
Cromarty, P. and Marks, I. (1995). Does rational role-play enhance the outcome of exposure therapy in dysmorphophobia? A case study. British Journal of Psychiatry, 167, 399-402.
de Oliveira, I.R. (2008). Trial-based thought record (TBTR): preliminary data on a strategy to deal with core beliefs by combining sentence reversion and the use of an analogy to a trial. Revista Brasileira de Psiquiatria, 30(1), 12–18.
de Oliveira, I.R. (2011). Kafka’s trial dilemma: Proposal of a practical solution to Joseph K.’s unknown accusation. Medical Hypotheses, 77(1), 5-6.
de Oliveira, I.R. (2012a) Trial-Based Cognitive Therapy. Accepted entry in Common Language for Psychotherapy Procedures.
de Oliveira, I.R. (2012b) Trial-Based Thought Record. Accepted entry in Common Language for Psychotherapy Procedures.
de Oliveira, I.R. (2015). Trial-Based Cognitive Therapy: A Manual for Clinicians. New York: Routledge.
de Oliveira, I.R. (2016) Trial-Based Cognitive Therapy: Distinctive Features. London:Routledge.
de Oliveira, I.R., Duran, E.P. and Velasquez, M. (2012). A trans-diagnostic observation of the efficacy of the Trial-Based Thought Record in changing negative core beliefs and reducing self-criticism. NEI Psychopharmacoloy Congress, San Diego, October 18-21.
de Oliveira, I.R., Hemmany, C., Powell, V.B., Bonfim, T.D., Duran, E.P., Novais, N. et al., (2012). Trial-based psychotherapy and the efficacy of trial-based thought record in changing unhelpful core beliefs and reducing self-criticism. CNS Spectrums, 17(1), 16–23.
de Oliveira, I.R., Powell, V.B., Caldas, M., Seixas, C., Almeida, C., Bomfim, T. et al. (2012). Efficacy of the Trial-Based Thought Record (TBTR), a new cognitive therapy strategy designed to change core beliefs, in social phobia: A randomized controlled study. Journal of Clinical Pharmacy and Therapeutics, 37(3), 328-334.
Freeman, A., DeWolf, R. (1992). The 10 Dumbest Mistakes Smart People Make and How to Avoid them. New York: HyperPerennial.
Kafka, F. (1925/1998). The Trial. New York: Schoken Books.
Leahy, R.L. (2003). Cognitive therapy techniques. A practitioner’s guide. New York: Guilford Press.
Messer, S.B. (1992). A critical examination of belief structures in interpretive and eclectic psychotherapy. In J.C. Narcross and M.R. Goldfried (Eds.), Handbook of Psychotherapy Integration. New York: Basic Books.
Mitchell, S. (1988). Relational Concepts in Psychoanalysis. Cambridge, MP: Harvard University Press.
Powell, V.B., de Oliveira, O.H., Seixas, C., Almeida, C., Grangeon, M.C., Caldas, M., et al. (2013). Changing core beliefs with trial-based cognitive therapy may improve quality of life in social phobia: a randomized study. Revista Brasileira de Psiquiatria, 35(3), 243-247.
Stricker, G. (2010). Psychotherapy Integration. Washington D. C.: American Psychological Association.
Published July 12, 2016
